Diary of a (secondline) clinicianOne of the many ways in which organisations have attempted to slow the spread of COVID-19 is by preventing the entry of the people with active fevers from entering certain buildings. This is largely achieved through checking the temperatures of all who enter, barring entry to those who fail the thermometer's test. Of course there's a lot to say that this may be ineffective, due to the significant presymptomatic and asymptomatic transmission of SARS-CoV-2, the virus that has caused us so much pain these last few months. But this is not what I'm interested in today. "This is achieved by checking the temperatures of all who enter, barring entry to those who fail the thermometer's test." My hospital has been no exception to this, closing all but two entrances and stationing a nurse and security guard at each armed with infrared forehead thermometers, cool demeanours, and eerily identical small-talk repertoire: "Staff or visitor?" "Staff" [waving my tag] [reading the thermometer] "All clear, have a lovely day!" "You too!" Of course this bottleneck to entry meant lines of up to 30 people during peak hour waiting to be scanned to get in. It was a rare day indeed when I didn't overhear someone nearby in the line (spaced by social distancing markers on the ground 1.5m apart of course) make a joke about needing Aldi checkout operators (the German supermarket chain renowned for its ruthlessly efficient checkout system). "a nurse and security guard at each [entrance] armed with infrared forehead thermometers, cool demeanours, and eerily identical small-talk repertoire" This was, until one day two weeks ago, when despite arriving at work at my usual time there was almost no one in line. The reason became clear when I had to choose between two thermometer armed nurses (I chose the one on the Right because just like the right main bronchus she was more directly in line with my path, I daren't say whether either of the other two comparative features of the Right vs. Left main bronchi were present). What a great idea I thought, double staffing at peak times to manage demand, who could have thought such a thing possible in a public hospital? "despite arriving to work at my usual time there was almost no one in line" So imagine my surprise when last week my traversal of the hospital entrance was as unimpeded as a Livian's travel to contiguous Spain. A questioning glance at the lobby now devoid of nurses and manned by a lone security guard was met with a gesture upwards and a muffled phrase through his facemask "Infrared mate". Now this was technology! Sure Singapore's Changi airport's been doing it for at least 10 years from what I remember of transits through it, but even so, unencumbered entry and protection from febrile people couldn't be any better than this. It wasn't until the third day of this that I overheard a nurse at the visitor registration bay, at which of course I'd never had to stop, mention that her colleague had picked up some screening shifts at The Austin, a nearby tertiary hospital, because "we had no work for her anymore". And there it was, in the space of a few weeks we'd recapitulated hundreds of years of human history. A new market identified, technology invented to service it that requires labour, rural to urban migration to provide the labour, boosting productivity, then further technological advancements that disrupt the industry and obviate the need for labour at all. Or perhaps I was reading too much into things, a fever dream. Maybe those infrared thermometers need checking... 
0 Comments
Diary of a (secondline) clinicianIt is a truth universally acknowledged in the internet age that an event noted by at least two people will soon become a meme. And I don't mean a meme in the true definitional sense, but the sense that language purists hate us all for, some mash-up of an over-used picture with heading text that commits all sort of type-setting and often a few grammar sins. So when the greatest existential threat to modern life as we know it came along, the memes virtually wrote themselves. "some mash-up of an over-used picture with heading text that commits all sort of type-setting and often a few grammar sins" Memes about not being able to leave the house, memes about world leaders, memes about bats and pangolins, memes conflating virology and beer-brewing, and yes, innumerable memes about toilet paper. You would think then that these memes served some purpose, pushed us towards some common goal. And yet you don't have to look far to find people decrying the viral spread of these memes as something about which to be very concerned. Reports of racism and discrimination in memes is of course disturbing and even a pandemic is no excuse for hate of any form towards our fellow man. Beyond this, even seemingly harmless memes are denounced as 'making light of something that kills people' or as 'mocking those who've lost their lives' "You would think then that these memes served some purpose, pushed us towards some common goal." But as one of my favourite childhood authors described, we are very good at rapidly making the extraordinary seem ordinary, in order to deal with it. Human cerebral adaptation, better known as just getting on with things is one of the remarkable features of human imagination that set us apart from other mammals. Thus memes, offensive as they may be to some, could be conceived as a way of normalising the COVID-19 pandemic in order to cope with it. If it's something we can make light of using internet culture in the same way we seem to make light of everything these days, then it's something we can deal with, and no longer the imminent existential threat that stuns us all into inaction. Discussions about the balance between speech freedom and the risk of being offended aside, COVID-19 memes are likely a sign of the human race adapting to and dealing with the set of circumstances few of us have previously found ourselves in. Whatever else you may say about humans, we're rather good at adapting.  Diary of a (secondline) clinicianA novel threat requires a co-ordinated response, of that there is no doubt. As we face such a threat it is more important than ever that we ensure our actions are optimal, as a medical profession, health system, and society. And as every high school student on a leadership or team-building course knows, the key is communication (...and teamwork, sometimes leadership, occasionally initiative). "As we face such a threat it is more important than ever that we ensure our actions are optimal, as a medical profession, health system, and society." In times gone by this would be achieved through large plenary lectures, "getting all the right people in the room" and hashing things out the old-fashioned way. However, the current imperative for social distancing, giving rise to increased familiarity with teleconferencing, has meant it's all too easy to set up a Zoom or Webex and let people know about it. It seems that the old adage holds true, if you build it, they will come. And in the present climate of hunger for any information on all things COVID-19, come they do, usually in droves. The problem is separating the wheat from the chaff. When you receive an invitation to Royal Tertiary's Grand Round at which the Health Minister is speaking of course you want to tune in. But then St. Excellence is describing their early experience with plexibox intubation straight after, and you can't miss that. During that talk your inbox pings with the medical school's roundtable on changing to a virtual curriculum, and as a clinical educator you'd better attend. As soon as that's done it's the inter-hospital COVID morbidity and mortality meeting, and oh look, it's 6 p.m. It's some irony that I've attended more meetings per week during a time when we can't meet than in typical months during which we could! "The problem is separating the wheat from the chaff." However, unlike in other more heavily bureaucratised health sytems *cough* America *cough*, these meetings are largely of our own making as clinicians. So it is the usual grievance of "just let me do my job" is a small voice amidst the louder cries of "tell me everything". Perhaps it's because our country's health systems 'ain't seen nothing yet', perhaps our bureaucrats are better at getting out of the way in a crisis. Unending meetings won't solve the pandemic, but enough of the right ones just may give us a fighting chance of coming out the other end bruised to be sure but unbroken. 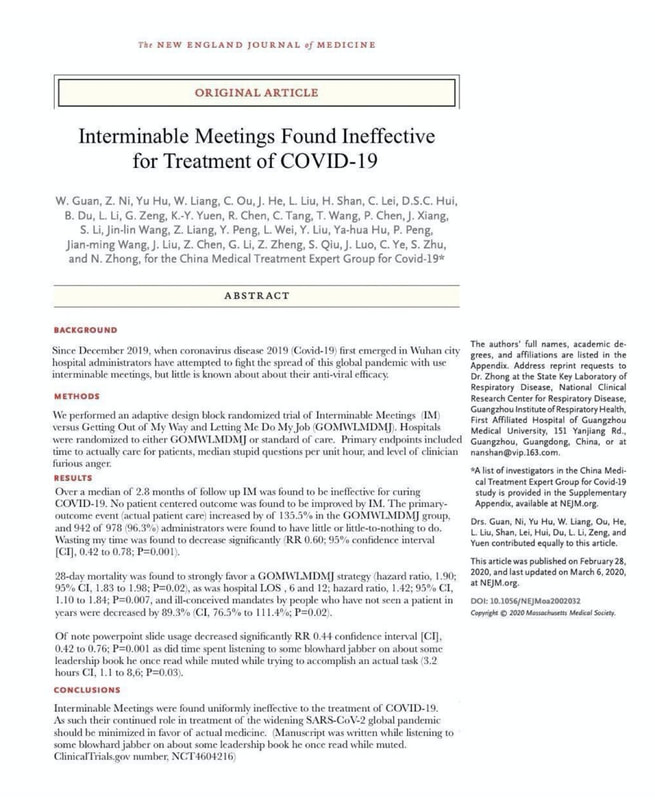 Diary of a (secondline) clinicianIt is well described that humans have multiple ways of thinking, one way of dichotomising these is into heuristic and analytic thought. Heuristic thinking is pattern recognition, once one has enough familiarity with a concept or circumstance one can immediately react appropriately to it without much further thought. This is like a brain reflex for when an immediate response is required. When a car is coming towards you down the wrong side of the road there's no need to think, it's time to run or jump out of the way. Analytic thinking is weighing up the pros and cons of various courses of action to decide on the best. Determining which courses to apply to study at university would be a good time to use this. "When a car is coming towards you down the wrong side of the road there's no need to think, it's time to run or jump out of the way" The heuristic thought mode is activated when time is of the essence such as when under threat or facing imminent danger. It's fast and where the situation is a familiar one, usually provides a good enough answer, based on experience. The analytic mode comes into its own when one has time and the consequences of the decision are significant, so an optimal decision is more important. It takes longer but is less likely to be biased by preconceptions and allows for a more complete consideration of the evidence. Healthcare professionals would do well to remember that in any medical context where one's health is at stake, but especially during a pandemic, patients feel under threat. Of course, this activates the heuristic thinking mode, where one doesn't have the brainspace to consider evidence. The fight or flight response activated, a brain simply wants to make a quick decision that will allow the body to escape the threat. No time for evidence and only one's prior experience to go on explains much of the otherwise irrational behaviour during trying times. "The analytic mode comes into its own when one has time and the consequences of the decision are significant" And so the great public health conundrum of how to pitch a message. At the mere suggestion of a new infection some anxious people are running for the hills while for others there would have to be bodies in the streets before they'd give up popping down to Dan Murphy's. Messages aimed at scaring the indifferent end of the spectrum into changing their behaviour are liable to induce panic in those at the anxious end. Similarly, when the public health information is attempting to calm panic-buying or mass flights away from infection epicentres, it runs the risk of overly reassuring those who need no extra reassurance. In the same way that those on the left and right of the political spectrum will interpret a news item in the most favourable way for their side of politics (a fact heavily exploited by news media), people will read into a public health message what they want to hear. Furthermore, it is impossible not to read into government policy and directives. - "The borders are closed and there's no pasta on the supermarket shelves, it must be the end of the world." - "The curve is flattening and hospitals aren't overwhelmed, there was nothing to worry about in the first place and all that social distancing has just screwed over the economy." I don't envy public health decisionmakers, almost as much as I don't envy politicians. If there was a way to target messaging to the individual that would be ideal, but well, we know how that worked out. So we are stuck with a heterogeneous public that must be simultaneously reassured and chastised. And all this to just the right degree to achieve the optimal overall pandemic response. A tall order indeed.  Diary of a (secondline) clinicianWhen the cat is away the mice come out to play. So it is with road use; when cars are off the road because far fewer people need to commute, cyclists and pedestrians are king. It's an odd feeling, to be able to cross the 6 lanes and 2 tram tracks between traffic lights of the main road I walk along to my hospital every morning. What's usually a veritable car park of vehicles heading into the city is now a deserted wasteland, one I can waltz across at my leisure. "It's an odd feeling, to be able to cross 6 lanes and 2 tram tracks between traffic lights of the main road" Unfortunately I still need to drive every so often, usually taking my wife to work at the weekends when she's charting chemo, saving lives, that sort of thing. The lack of other cars on the road is a definite plus and makes it almost disconcertingly easy to cross the city, usually a prolonged and frustrating trip. But you never get something for nothing. In the place of the usual maze of bumper to bumper traffic instead there are an inordinate number of pedestrians criss-crossing the roads. More than a few times I've had to take evasive action well away from a traffic light. Of course I'm very good at resolving any cognitive dissonance related to my own skylarking across 8 lanes in the morning by reassuring myself that I of course always make sure to never jaywalk in front of a car. For many years I thought jaywalking referred to crossing a road at the lights but rather than exiting at the correct spot, veering off to the left or right in one's eventual direction of travel, so tracing the letter "J" with one's path. Turns out it doesn't refer to this at all but rather a 'jay' being now out-of-use US slang for a person from the country. These jays when in Kansas City would treat the main streets as if they were country lanes, crossing the road anywhere they pleased, paying no heed to the many cars that would have to rapidly slow or stop to avoid injury. "More than a few times I've had to take evasive action well away from a traffic light" All of this of course begs the question whether disregard for motor vehicles will persist beyond our current pandemic/lockdown state and if this event will mark a watershed of pedestrians reclaiming the road from their motor vehicle nemeses. I suspect there will be some renegotiation of the new-found freedoms pedestrians currently enjoy that they will fight to keep. This will almost certainly be assisted by the likely long-lasting reduction in traffic we will see from an increased ability for people to work from home, espeically now that so many have (been forced to) experience it and found it adequate if not superior to commuting and being away from one's family. Perhaps a silver lining of our current experience shall be a win for our climate and planet.  |
DownloadsCheck out the downloads on the next page. Archives
May 2020
Categories |
 RSS Feed
RSS Feed
